































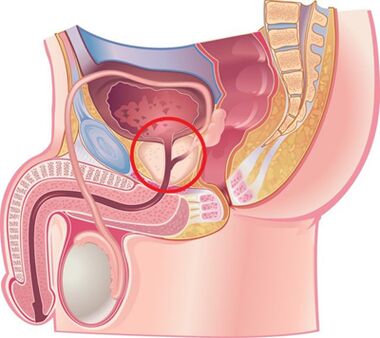
According to many experts, chronic prostatitis is an inflammatory disease, the cause of which is an infection with a possible accession of an autoimmune disorders, characterized by damage to the parenchymal and interstitial tissue of the organ.The disease has known medicine since 1850, but today it remains insufficiently studied and poorly treatable.Chronic bacterial (6 - 10%) and non -bacterial (80 - 90%) prostatitis are the most common and socially significant inflammatory diseases in men that significantly reduce their quality of life.The disease is recorded mainly in people of young and middle age and is often complicated by impaired copulation and generative functions (reduction of potency, infertility, etc.).The disease is recorded in men in 8 - 35% of cases aged 20 to 40 years.
The cause of bacterial prostatitis is pyogenic flora that penetrates the gland from the urethra, or through the lymphogenous and hematogenous routes.The etiology of chronic nonbacterial prostatitis and its pathogenesis remain unknown.It affects mainly men over 50 years of age.
The causes of the development of the disease
Chronic prostatitis is currently considered as a polyetiological disease.There is an opinion that the disease occurs as a result of the penetration of infection into the prostate, and then the pathological process proceeds without its participation.This is facilitated by a number of non -infectious factors.
Infectious factors in the development of chronic prostatitis
In 90% of cases, pathogens penetrate the iron from the urethra, as a result of which acute or chronic prostatitis occurs.Cases of asymptomatic carriage are noted.The course of the disease is influenced by the state of the protective forces of the human body and the biological properties of the pathogen.It is assumed that the transition of acute prostatitis to chronic occurs due to loss of tissue elasticity due to excess products of fibrous tissue.
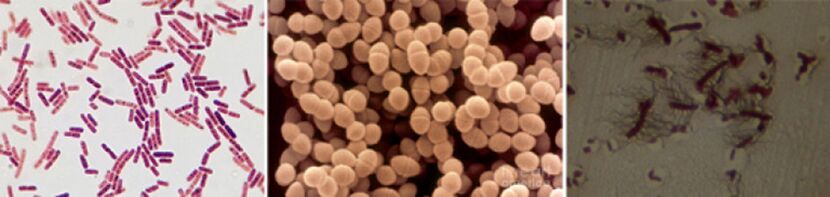
The following pathogens are found among the causative agents of chronic prostatitis:
- In 90% of cases, the disease reveals gram-negative bacteria such as Escherichia coli (Escherichia coli), Enterococcus faecalis (fecal enterococcus), and somewhat less frequently - Pseudomonas aeruginosa, Klebsiella spp., Proteus spp.,Pseudomonas aeruginosa, Enterobacter aerogenes and Acinetobacter spp.Gram-positive bacteria enterorococci, streptococci and staphylococci are rare.
- The role of coagulase-negative staphylococci, ureaplasma, chlamydia, trichomonas, gardnerella, anaerobic bacteria and fungi of the genus Candida has not been fully elucidated.
The infection into the prostate penetrates in several ways:
- The ascending path is the most probable that is proved by a frequent combination of prostatitis and urethritis.
- Hematogenous prostatitis develops when infection penetrates into the gland through the bloodstream, which is observed in chronic tonsillitis, sinusitis, periodontitis, pneumonia, cholecystitis and cholangitis, purulent skin diseases, etc.
- By contact, chronic prostatitis develops with urethritis and urethral strictures, when the infection penetrates the gland ascendingly with urine flow, with purulent kidney infections, canalicularly with epipidymitis, deferentitis and funiculitis, during diagnostic and therapeutic urological manipulations (catheterization, bougienage, urethral instillation),including transurethral.
- Lymphogenously, the infection penetrates into the prostate during proctitis, thrombophlebitis of hemorrhoidal veins, etc.
Non-infectious factors in the development of chronic prostatitis
Chemical factors
According to experts, the leading role in the development of chronic prostatitis belongs to intraprostatic urine reflux, when urine flows from the urethra into the gland, which leads to impaired emptying of the prostate and seminal vesicles.
With the disease, vascular reactions develop to the edema of the organ, the nervous and humoral regulation of the tone of the smooth muscle tissues of the urethra, and the activation of the alpha are disturbed1-adrenergic receptors causes the development of dynamic obstruction and contributes to the development of new intraprostatic refluxes.
During reflux, urates contained in urine lead to the development of a “chemical inflammatory response.”
Hemodynamic disorders
Support chronic inflammation of circulatory disorders in the pelvic organs and scrotum.Stagnation develops in persons leading a sedentary lifestyle, for example, for drivers, office employees, etc., with obesity, sexual withdrawal, sexual sex dysmetry, frequent hypothermias, mental and physical overloads.Maintaining the inflammatory process, taking spicy and spicy foods, alcohol and smoking, etc.
Other factors
There are many other factors that support chronic inflammation in the prostate.These include:
- Hormonal.
- Biochemical.
- Immune response disorders.
- Autoimmune mechanisms.
- Infectious and allergic processes.
- Features of the structure of the prostate glands, leading to difficulty in proper drainage.
Quite often, it is not possible to establish the causes of chronic prostatitis.
Classification of prostatitis
According to the classification proposed in 1995 by the US National Institutes of Health, prostatitis is divided into:
- Sharp (category I).Is 5 - 10%.
- Chronic bacterial (category II).Is 6 - 10%.
- Chronic non-bacterial inflammatory (category IIIA).It is 80 - 90%.
- Chronic non-bacterial non-inflammatory (category IIIB) or chronic pelvic pain syndrome.
- Chronic prostatitis detected by accident (category IV).
Signs and symptoms of chronic prostatitis
The course of chronic prostatitis is long, but not monotonous.Periods of exacerbation are followed by periods of relative calm, which occur after complex anti-inflammatory and antibacterial therapy.
The development of chronic bacterial prostatitis is often preceded by urethritis of bacterial or gonorrhea nature, non -bacterial - circulatory disorders in the pelvic organs and scrotum (hemorrhoids, varicocells, etc.), sexual excesses.
Patients with chronic prostatitis present many complaints.They have been going to doctors for years, but are very rarely examined for prostate disease.About a quarter of patients do not have any complaints, or the disease occurs with scanty clinical symptoms.
Complaints from patients with chronic prostatitis can be divided into several groups.
Urination disturbances associated with narrowing of the urethra:
- Difficulty initially urinating.
- Weak stream of urine.
- Intermittent or urination dropped.
- Feeling of incomplete emptying of the bladder.
Symptoms caused by irritation of nerve endings:
- Frequent urination.
- The urge to urinate is sharp and strong.
- Urination in small portions.
- Urine incontinence during the urge to urinate.
Pain syndrome:
- The intensity and nature of the pain varies.
- Localization of pain: lower abdomen, perineum, rectum, groin and lower back, inner thighs.
Sexual dysfunction:
- Pain in the rectum and in the urethra during ejaculation.
- Sluggish erection.
- Loss of orgasm.
- Premature ejaculation, etc.
From the nervous system: neurotic disorders in the form of fixing the attention of patients in the state of their health.
Signs and symptoms of chronic non -bacterial prostatitis
Chronic pelvic pains in men (CFTB) proceeds with the usual symptoms for chronic prostatitis, but in the 3rd portion of urine and a secret of the prostate in the study of the bacteria are absent.Simulate CTB can simulate chronic nebacterial interstitial cystitis, diseases of the rectum, spastic pelvic floor spastic myalgia and a functional prostate caused by impaired organic organ innervation and its hemodynamics.
In case of impaired neurovegetative function, atony and impaired innervation of the gland are noted, which is manifested by difficulties of the rapid and complete closure of the lumen of the urethra.At the same time, urine, after urination, continues to stand out for a long time drops.In such patients, in the study, instability and increased excitability are found, which is manifested by increased sweating and excitability of cardiac activity, changes in dermographism.

Complications of the disease
The long course of chronic prostatitis is complicated by disorders of sexual and reproductive functions, the development of diseases such as vesiculite and epipidimitis, as well as sclerosis of the organ.The sclerosion of the organ worsens local microcirculation and urodynamics, as well as the results of surgical interventions.Fibrosis of perihumetral tissues leads to the development of urination disorders.
Diagnostics
Due to the fact that there are many reasons for the development of chronic prostatitis, a whole range of diagnostic tests is used to diagnose it.The success of treatment depends on the correct identification of the causes of the disease.Diagnosis of chronic prostatitis is based on the following data:
- Classic triad of symptoms.
- A complex of physical methods (finger rectal examination of the prostate).
- A set of laboratory methods (urinalysis and microscopy of prostate secretions, culture and determination of the sensitivity of microflora to antibacterial drugs, general analysis of urine and blood).
- To detect gonococci, bacterioscopy smear from urethra, PCR and serological methods (for detecting ureaplasmes and chlamydia).
- Urofluometry.
- Prostate biopsy.
- A set of instrumental methods (ultrasound examination).
- Determination of the patient's immune status.
- Determination of neurological status.
- With the ineffectiveness of treatment and suspicion of the development of complications, computed and magnetic resonance imaging, blood sowing, etc.
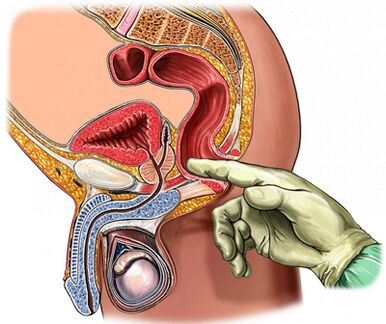
Palpation of the prostate gland
Of primary importance in diagnosing the disease is palpation of the prostate, which increases during the period of exacerbation and decreases during the period of subsidence of the inflammatory process.In chronic prostatitis, during the period of exacerbation, the gland becomes swollen and painful.
The consistency of the organ can be different: areas of softening and hardening are palpated, and areas of retraction are determined.By palpation it is possible to assess the shape of the gland, the condition of the seminal tubercles and surrounding tissues.
The process of transrectal finger examinations is combined with the seizure of the gland.Sometimes there is a need to get a secret from each share separately.
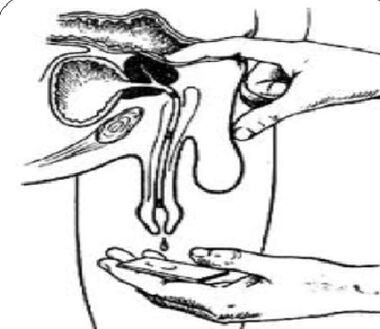
Analysis of a 3-cup sample of urine and prostate secretion
The “gold standard” in the diagnosis of chronic prostatitis are:
- Collection of the first portion of urine.
- Collection of a second portion of urine.
- Obtaining gland secretions through massage.
- Collection of the third portion of urine.
Next, microscopic and bacteriological examination of the material is carried out.
For inflammation of the prostate:
- Microbial count (CFU) exceeds 103/ml (104/ml for epidermal staphylococci), but should not be neglected by a small number of microbes calculated by dozens and hundreds.
- The presence of 10-15 leukocytes in the field of view detected by microscopy is a generally accepted criterion for the presence of an inflammatory process.
The secret of prostate and 3rd portions of urine are subjected to microscopic and bacteriological studies:
- In chronic bacterial prostatitis, an increase in the number of leukocytes in the secret of the gland and the third post -massage portion of urine is noted, bacteria (mainly intestinal group) are released.
- With non-bacterial prostatitis, there is an increase in the number of leukocytes in the secretion of the gland, but the microflora is not detected.
- With CTB, there are no increased amounts of white blood cells and microflora.
The normal indicator of the secret of the prostate:
- Less than 10 leukocytes per field of view.
- There is a large amount of lecithin grains.
- There is no microflora.
In chronic prostatitis in the secret of the prostate, it is found:
- The number of leukocytes is large-exceeds 10-15 in the field of view.
- The number of lecithin grains is reduced.
- The pH of the secretion shifts to the alkaline side.
- The content of acid phosphatase is reduced.
- Lysozyme activity is increased.
Obtaining negative results of the secret of the prostate once does not prove the lack of an inflammatory process.
The value of the test of the secret of the prostate remains.Normally, during crystallization, a characteristic pattern is formed in the form of a fern sheet.In case of violation of the aggregation properties of the prostatic secret, such a pattern does not form what occurs with changes in the androgenic hormonal background.
Ultrasound study
In case of suspicion of prostate disease, an ultrasound examination of the gland itself is used (transiental ultrasound), kidneys and bladder is optimal, which allows you to determine:
- Volume and size of the gland.
- The presence of calculi.
- Sizes of seminal vesicles.
- Condition of the bladder walls.
- Amount of residual urine.
- Clothing structures.
- Another type of pathology.
Other prostate research methods
- The state of urodynamics (the study of urine flow rate) is easily and simply determined using a study such as uroflowmetry.With the help of this study, it is possible to promptly detect signs of bladder outlet obstruction and carry out dynamic monitoring.
- A puncture biopsy is performed if abscess formation, benign hyperplasia and prostate cancer are suspected.
- In order to clarify the causes of the development of infravezicular obstruction, radiological and endoscopic examination is carried out.
- With a long -flowing inflammatory process, it is recommended to carry out urethrocystoscopy.
Differential diagnosis
Chronic prostatitis should be distinguished from vesiculoprofeostasis, autonomic prostatopathy, stagnant prostatitis, pelvic bottom, psychoneurological disorders, pseudo -detission, reflex sympathetic dystrophy, inflammatory diseases of other organs: interstitial cystitis, osteitis of the longitudinal art, sexual dysphuncture, sexual dysphuncture, sexual dysphuncture, sexual dysfunction.Hypertrophy of the neck of the bladder, strictures of the urethra, tuberculosis, prostate cancer and bladder, urolithiasis, chronic epipidimite, inguinal hernia.
Treatment of chronic prostatitis
Treatment of chronic prostatitis should begin with a change in the lifestyle and nutrition of the patient.
When treating the disease, medications that affect different parts of the pathogenesis are simultaneously used.
The main directions of therapy:
- Elimination of causative microorganisms.
- Anti-inflammatory therapy.
- Normalization of blood circulation in the prostate and pelvic organs.
- Normalization of adequate drainage of prostatic acinus.
- Normalization of the hormonal profile.
- Prevention of organ sclerosion.
For the treatment of chronic prostatitis, drugs of the following groups are used:
- Antibacterial.
- Anticholinergic.
- Vasodilators.
- Alpha1–Adren -blocking.
- 5 alpha reductase inhibitors.
- Cytokine inhibitors.
- Non -steroidal anti -inflammatory.
- Angioprotectors.
- Immunomodulators.
- Preparations affecting the exchange of urates.
Antibiotics in the treatment of bacterial chronic prostatitis
Antibacterial therapy should be carried out taking into account the sensitivity of detected microorganisms to antibiotics.In the case of non -detection of the pathogen, empirical antimicrobial treatment is used.
The drugs of choice are fluoroquinolones of the II - IV generation.They quickly penetrate into the tissues of the gland with ordinary methods of use, show activity against a large group of gram -negative microorganisms, as well as ureaplasma and chlamydia.In case of failure of antimicrobial treatment, it should be assumed:
- Microflora polyurezancy,
- short (less than 4 weeks) treatment courses,
- Incorrect selection of the antibiotic and its dosage,
- changes in the type of pathogen,
- The presence of bacteria that live in the ducts of the prostate, covered with a protective extracellular membrane.
The duration of treatment should be at least 4 weeks with the obligatory subsequent bacteriological control.In case of preservation in the 3rd portion of urine and the secret of the prostate of bacteriuria more than 103CFU/ml a repeat course of antibacterial therapy is prescribed for a period of 2 to 4 weeks.
Cytokine inhibitors in the treatment of chronic prostatitis
Cytokines are glycoproteins that are secreted by immune and other cells in conditions of inflammatory reaction and an immune response.They take an active part in the development of a chronic inflammatory process.
Nonsteroidal anti -inflammatory drugs
Non -steroidal anti -inflammatory drugs have an anti -inflammatory effect, reduce pain and fever.They are widely used in the treatment of chronic prostatitis in the form of tablets and suppositories.The most effective is the rectal path of introduction.
Immunotherapy
In the treatment of bacterial chronic prostatitis, in addition to antibiotics and anti -inflammatory drugs, immunomodulating agents are used.The most effective is the rectal path of their introduction.The immunomodulator is widely used, which increases the functional activity of phagocytes, which contributes to a more effective elimination of pathogens.
Alpha-blockers in the treatment of chronic prostatitis
It was established that alpha-1 adrenergic shoes normalize the tone of the smooth muscles of the prostatic part of the urethra, seed bubbles and prostate capsules, which makes drugs of this group very effective in the treatment of the disease.Alpha-1 adrenergic shoes are used in patients with pronounced urination disorders in the absence of an active inflammatory process.
For CPPS, the treatment period ranges from 1 to 6 months.
5a-reductase inhibitor in the treatment of abacterial prostatitis and CPPS
It has been established that under the influence of the enzyme 5a-reductase, testosterone is converted into the prostatic form 5a-dihydrotestosterone, the activity of which in prostate cells is more than 5 times higher than the activity of testosterone itself, which in elderly people leads to an enlargement of the organ due to the epithelial and stromal components.
When taking a 5a-reductase inhibitor, atrophy of stromal tissue is observed for 3 months, glandular tissue atrophy for 6 months, secretory function is inhibited, the severity of pain and the volume of the gland are reduced, tension and swelling of the organ are reduced.
The role of anti -sclerotic drugs in the treatment of chronic prostatitis
With a long -flowing inflammation in the prostate gland, fibrosis develops, which is manifested by disorders of microcirculation and urodynamics.In order to prevent the process of fibrification, anti -sclerotic drugs are used.
Other drugs used in the treatment of chronic prostatitis
Along with the above drugs, the disease is used to treat the disease:
- Antihistamines.
- Vasodilators and angioprotectors.
- Immunosuppressants.
- Preparations that affect the exchange of urates and trinatrium salt of citric acid.
Herbal products
Effective in the treatment of prostatitis, the use of the drug in the form of candles containing a complex of biologically active peptides isolated from the prostate gland of cattle.
Under the influence of the drug occurs:
- Stimulation of metabolic processes in the tissues of the gland.
- Improving microcirculation.
- Reducing edema, leukocyte infiltration, stagnation and pain.
- Prevention of thrombosis in the venules of the prostate gland.
- Increased activity of the secretory epithelium of the acini.
- Improving sexual function (increased libido, restoration of erectile function and normalization of spermatogenesis).
Finger massage of the prostate gland
A number of researchers say that in chronic prostatitis, a finger massage should be used, taking into account known contraindications.
Physiotherapy
The effectiveness of physiotherapeutic procedures in the treatment of prostatitis is not proven today, the mechanism of action has not been scientifically established, adverse reactions have not been studied.
Prevention of chronic prostatitis
Starting the prevention of the development of chronic prostatitis, you should know:
- The risk of developing the disease increases with age.
- Representatives of the Negroid race are more predisposed to the disease.
- A family predisposition to the disease is not excluded.
Persons with a predisposition to the development of chronic prostatitis should be more attentive to their state of health.
Disease prevention tips:
- Take enough fluids.Frequent urination helps flush out microflora from the urethra.
- Prevent diarrhea and constipation.
- Adhere to a rational diet.Do not eat food saturated with carbohydrates and saturated fats, which leads to an increase in body weight.
- It should be limited to the use of substances that irritate the urethra: sharp and spicy dishes, smoked meats, sauces and seasonings, coffee and alcohol.
- Refuse smoking.Nicotine negatively affects the condition of the vascular walls.
- Don't get too cold.
- Do not hold the emptying of the bladder.
- Lead an active lifestyle, play sports.Do the exercises to strengthen the muscles of the pelvis, which allows you to eliminate stagnation of venous blood, which, in turn, supports the normal function of the prostate gland.
- Lead regular sex life.Avoid prolonged abstinence.Iron should be freed in a timely manner from the secret.
- Stay adherents of monogamous relations.Illegal sexual relations increase the likelihood of acquiring sexually transmitted diseases.
- If complaints appear by the genitourinary authorities, immediately contact a urologist.
